Indication
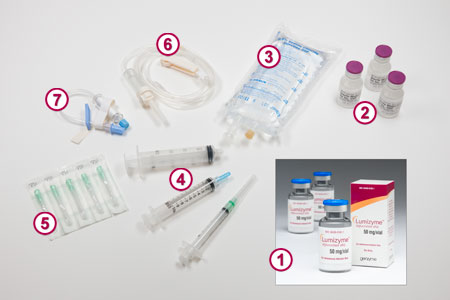
LUMIZYME® (alglucosidase alfa) is a hydrolytic lysosomal glycogen-specific enzyme indicated for patients with Pompe disease (GAA deficiency).
Important Safety Information
WARNING: HYPERSENSITIVITY REACTIONS INCLUDING ANAPHYLAXIS, IMMUNE-MEDIATED REACTIONS, AND RISK OF ACUTE CARDIORESPIRATORY FAILURE
Hypersensitivity Reactions Including Anaphylaxis
Patients treated with LUMIZYME have experienced life-threatening hypersensitivity reactions, including anaphylaxis. Appropriate medical monitoring and support measures, including cardiopulmonary resuscitation equipment, should be readily available during LUMIZYME administration. If a severe hypersensitivity reaction (e.g. anaphylaxis) occurs, discontinue LUMIZYME immediately and initiate appropriate medical treatment.
Consider risks and benefits of re-administering LUMIZYME following severe hypersensitivity reactions. If a mild or moderate hypersensitivity reaction occurs, the infusion rate may be slowed or temporarily stopped. Prior to LUMIZYME administration, consider pretreating with antihistamines, antipyretics, and/or corticosteroids.
Immune-Mediated Reactions
Immune-mediated reactions presenting as proteinuria, nephrotic syndrome, and necrotizing skin lesions have occurred in some patients following LUMIZYME treatment. Monitor patients for the development of systemic immune-mediated reactions involving skin and other organs while receiving LUMIZYME.
Risk of Acute Cardiorespiratory Failure
Infantile-onset Pompe disease patients with compromised cardiac or respiratory function may be at risk of serious acute exacerbation of their cardiac or respiratory compromise due to fluid overload and require additional monitoring.
Infusion Associated Reactions (IARs): Infusion Associated Reactions (IARs) have been observed in patients treated with Lumizyme. Discontinue immediately or adjust the infusion rate and provide medical treatment based on the severity of the reaction. Closely monitor patients who have experienced IARs when re-administering LUMIZYME.
Risk of Cardiac Arrhythmia and Sudden Cardiac Death during General Anesthesia for Central Venous Catheter Placement: Caution should be used when administering general anesthesia for the placement of a central venous catheter intended for LUMIZYME infusion.
Risk of Antibody Development: Patients with Infantile-onset Pompe disease should have a cross-reactive immunologic material (CRIM) assessment early in their disease course and be managed by a specialist knowledgeable in immune tolerance induction in Pompe disease to optimize treatment. Evidence suggests that patients who develop high and sustained IgG antibody titers may experience reduced clinical efficacy.
Monitoring: Laboratory Tests: Patients should be monitored for IgG antibody formation every 3 months for 2 years and then annually thereafter. Patients who experience hypersensitivity reactions, including anaphylaxis, may also be tested for IgE antibodies to LUMIZYME and other mediators of anaphylaxis.
Adverse Reactions
The most frequently reported adverse reactions (≥ 5%) in clinical trials were hypersensitivity reactions and included: anaphylaxis, rash, pyrexia, flushing/feeling hot, urticaria, headache, hyperhidrosis, nausea, cough, decreased oxygen saturation, tachycardia, tachypnea, chest discomfort, dizziness, muscle twitching, agitation, cyanosis, erythema, hypertension/increased blood pressure, pallor, rigors, tremor, vomiting, fatigue, and myalgia.
Please see the Full Prescribing Information for complete details, including boxed WARNING.